Lipedema and lymphedema are chronic medical conditions that affect the limbs and body tissues, often causing swelling, discomfort, and changes in body contour. Although the names sound similar, these two disorders involve different underlying mechanisms and treatments.
Many patients are initially misdiagnosed because both conditions can cause enlargement of the legs or arms. However, lipedema primarily involves abnormal fat accumulation, while lymphedema results from impaired lymphatic drainage and fluid buildup.
Understanding the difference between these conditions is important because treatment strategies vary significantly.
1 of 6
Lipedema is a chronic adipose tissue disorder characterized by abnormal and symmetrical accumulation of fat, most commonly affecting the legs, thighs, hips, buttocks, and sometimes the arms.
The condition primarily affects women and often develops or worsens during hormonal changes such as puberty, pregnancy, or menopause.
Common Symptoms of Lipedema
Patients with lipedema often experience:
A key feature of lipedema is that the feet and hands are usually spared, resulting in a visible “ankle cuff” or “wrist cuff.”
Lymphedema is a condition caused by impaired lymphatic drainage, which leads to the accumulation of protein-rich lymphatic fluid in the tissues.
The lymphatic system plays a critical role in fluid balance and immune function. When lymphatic vessels are damaged or blocked, fluid can accumulate in the surrounding tissues.
Lymphedema may occur due to:
Unlike lipedema, lymphedema may affect one limb or one side of the body.
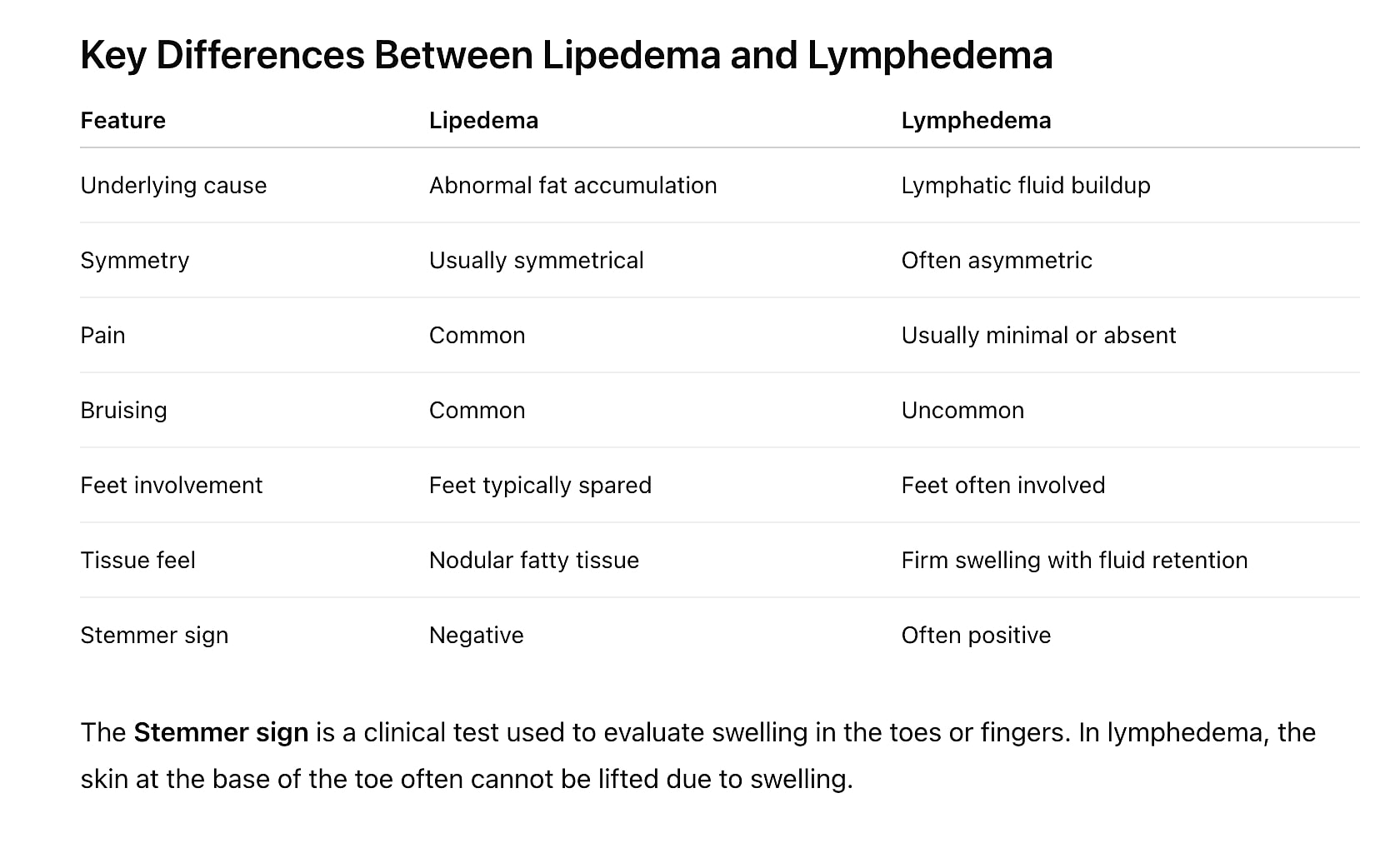
Although lipedema and lymphedema can both cause enlargement of the limbs, the symptoms and physical findings are different. Recognizing these differences can help physicians determine the underlying cause of swelling and guide appropriate treatment.
Common Symptoms of Lipedema
Lipedema is a chronic adipose tissue disorder characterized by abnormal fat accumulation, most commonly affecting the legs, hips, buttocks, and sometimes the arms. The condition almost exclusively affects women and often develops during periods of hormonal change.
Typical symptoms of lipedema include:
The affected tissue often feels soft but nodular, and patients frequently report that the limbs are painful when pressed.
Common Symptoms of Lymphedema
Lymphedema occurs when the lymphatic system is unable to properly drain lymphatic fluid, leading to fluid accumulation in the tissues. This condition may occur after lymph node removal, radiation therapy, trauma, infection, or congenital lymphatic abnormalities.
Common symptoms of lymphedema include:
In early stages, the swelling may be soft and pitting, meaning the tissue temporarily indents when pressed. Over time, chronic inflammation may cause fibrosis and tissue thickening.
Lipedema is frequently mistaken for:
However, lipedema fat deposits are resistant to weight loss, and patients often report persistent pain and tenderness, which are less common in other conditions.
Early recognition is important because untreated lipedema can progress over time and may eventually lead to secondary lymphedema, sometimes referred to as lipo-lymphedema.
The diagnosis of lipedema and lymphedema typically begins with a comprehensive clinical evaluation, including a detailed medical history and physical examination. Because these conditions can appear similar, careful assessment is necessary to distinguish between abnormal adipose tissue disorders and lymphatic dysfunction.
During the examination, physicians evaluate several important clinical features, including:
In lipedema, fat accumulation typically occurs in a symmetrical pattern involving the legs, thighs, hips, buttocks, and sometimes the arms, while the hands and feet are usually spared, creating a characteristic “cuff” appearance at the ankles or wrists. Patients often report tenderness, easy bruising, and pain within the affected tissues, which are less common in lymphedema.
In contrast, lymphedema results from impaired lymphatic drainage, leading to the accumulation of lymphatic fluid within the tissues. Swelling may occur in one limb or asymmetrically, and the hands or feet are frequently involved. The skin may become thickened over time, and a clinical finding known as the Stemmer sign—inability to pinch the skin at the base of the toes or fingers—may be present.
Imaging studies may be used in certain cases, especially for lymphedema, to further evaluate the lymphatic system or exclude other causes of swelling. These studies may include:
Although imaging can provide additional information, lipedema is most often diagnosed clinically based on the patient’s symptoms and physical findings. Imaging is typically used to confirm suspected lymphedema, evaluate lymphatic dysfunction, or rule out other causes of limb enlargement.
Accurate diagnosis is essential because lipedema and lymphedema require different treatment strategies, and early recognition can help guide appropriate management.

In some patients, long-standing lipedema may eventually lead to secondary lymphatic dysfunction, a condition commonly referred to as lipo-lymphedema.
Over time, the progressive enlargement of lipedema adipose tissue can place increased pressure on lymphatic vessels, impairing their ability to transport lymphatic fluid. When this occurs, the patient may develop features of both lipedema and lymphedema.
Patients with lipo-lymphedema may experience:
The development of lipo-lymphedema can significantly worsen symptoms and may lead to functional limitations and increased risk of skin infections.
Early recognition and management of lipedema may help reduce the risk of progression to lipo-lymphedema and guide appropriate treatment strategies.

Treatment for lipedema focuses on reducing symptoms and improving function.
Conservative management may include:
In selected patients, lipedema reduction surgery using lymphatic-sparing liposuction techniques may help reduce the burden of diseased adipose tissue and improve symptoms.
These procedures are designed to remove abnormal adipose tissue while preserving lymphatic structures.

Management of lymphedema focuses on reducing limb swelling, improving lymphatic drainage, and preventing progression of the disease. Treatment typically begins with conservative therapies aimed at controlling fluid accumulation and supporting lymphatic circulation.
Non-Surgical Treatment
Common non-surgical treatments include:
These therapies are particularly helpful in early-stage lymphedema, when swelling is primarily due to the accumulation of lymphatic fluid.
Surgical Treatment Options
In some patients, particularly those with chronic or advanced lymphedema, surgical treatment may be considered when conservative therapies alone do not sufficiently control symptoms.
Surgical options may include:
Treatment strategies for lymphedema are typically individualized, and optimal management often involves a multidisciplinary approach combining conservative therapy with selected surgical options when appropriate.
In chronic or advanced lymphedema, the enlargement of the limb is often not caused solely by fluid accumulation. Over time, lymphatic dysfunction can stimulate the development of excess adipose (fat) tissue within the affected limb, which contributes significantly to the increased limb volume.
When this fibrofatty tissue component becomes dominant, conservative therapies alone may not adequately reduce limb size.
In these cases, liposuction-based debulking procedures have become an established surgical treatment option. Liposuction can remove the excess adipose tissue that develops in chronic lymphedema and significantly reduce limb volume. Studies have shown that chronic non-pitting lymphedema of the arm or leg can be effectively treated with liposuction, with substantial volume reduction often occurring within the first few months after surgery.
Modern techniques frequently use energy-assisted liposuction technologies such as ultrasound-assisted liposuction (VASER), which helps break up fibrotic tissue and facilitates removal of hypertrophied fat deposits that develop in long-standing lymphedema.
Research has demonstrated that liposuction-based treatments can significantly reduce limb volume in both upper and lower extremities and may improve quality of life and decrease infection rates associated with chronic lymphedema.
Patients undergoing liposuction treatment for lymphedema typically require continued use of compression therapy after surgery to maintain long-term results.
In some patients, particularly those with earlier-stage disease, microsurgical procedures designed to restore lymphatic drainage may be considered. These procedures may include:
In certain specialized centers, liposuction may be combined with these procedures to address both excess adipose tissue and lymphatic dysfunction simultaneously.
Individualized Treatment
Treatment strategies for lymphedema are highly individualized and depend on:
Optimal management often involves a multidisciplinary approach combining conservative therapy with selected surgical interventions when appropriate.
Patients who experience persistent swelling, pain, or progressive enlargement of the legs or arms should seek evaluation by a physician experienced in lymphatic and adipose tissue disorders.
Early diagnosis can help guide treatment and may prevent progression of symptoms.
Although lipedema and lymphedema may appear similar, they represent distinct medical conditions with different causes and treatments.
Accurate diagnosis allows physicians to develop a personalized treatment plan that addresses the underlying condition and improves patient quality of life.
Accurate diagnosis of lipedema and lymphedema requires experience in evaluating both adipose tissue disorders and lymphatic conditions. Dr. Emmanuel De La Cruz provides specialized evaluation and treatment for patients with limb enlargement, swelling, and abnormal fat distribution.
Key reasons patients choose Dr. De La Cruz include:
Patients seeking evaluation for lipedema vs lymphedema benefit from a comprehensive assessment that focuses on accurate diagnosis, evidence-based treatment, and personalized care.
In advanced stages, lipedema can impair lymphatic drainage and lead to secondary lymphedema, sometimes referred to as lipo-lymphedema.
Weight loss may improve overall health but typically does not eliminate lipedema fat deposits, which behave differently from normal adipose tissue.
Lipedema often runs in families, suggesting a genetic component.
Yes. Although the legs are most commonly affected, lipedema may also involve the upper arms and trunk.
Lymphedema is usually a chronic condition, but symptoms can often be managed effectively with proper treatment.
Lipedema is frequently misdiagnosed because its symptoms can resemble other conditions that cause enlargement of the limbs, including obesity, lymphedema, or chronic venous insufficiency. Unlike obesity, however, lipedema fat deposits are often resistant to diet and exercise, and patients commonly experience pain, tenderness, and easy bruising in the affected areas. Additionally, the characteristic pattern of fat distribution—typically involving the legs, hips, buttocks, and sometimes the arms while sparing the hands and feet—may not be immediately recognized. Because awareness of lipedema has historically been limited, many patients experience delays in diagnosis before being evaluated by specialists familiar with the condition.
Liposuction can be used as a treatment option for selected patients with lipedema, particularly when symptoms persist despite conservative management. Lymphatic-sparing liposuction techniques are designed to remove abnormal lipedema adipose tissue while preserving surrounding lymphatic structures. By reducing the volume of diseased fat, liposuction may help improve symptoms such as pain, heaviness, and mobility limitations, while also improving body contour. Although liposuction does not cure the underlying disease process, it may significantly reduce the burden of lipedema tissue and improve quality of life for appropriately selected patients.
In certain cases of chronic or advanced lymphedema, liposuction may be used to reduce limb volume. Over time, long-standing lymphedema can lead to the development of fibrofatty tissue within the affected limb, which contributes to persistent enlargement even when fluid accumulation is controlled. Liposuction techniques, including ultrasound-assisted approaches such as VASER liposuction, can remove this excess adipose tissue and reduce limb size in selected patients. Following surgery, patients typically continue compression therapy to maintain long-term results. Treatment decisions depend on the stage of the disease and the underlying cause of the lymphatic dysfunction.
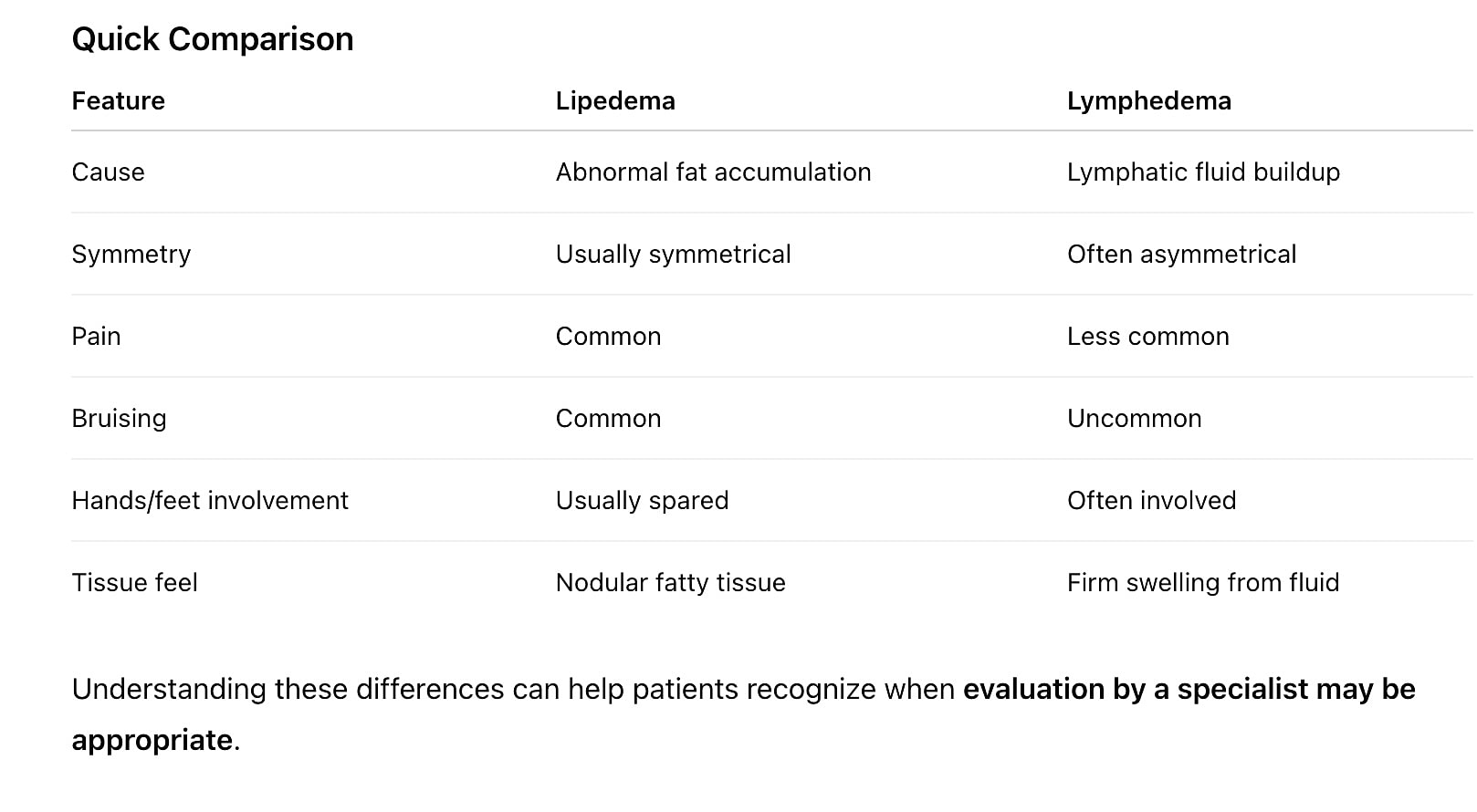
Several clinical features help distinguish between these two conditions. Lipedema typically causes symmetrical enlargement of the legs or arms and is often associated with pain, tenderness, and easy bruising. The hands and feet are usually spared, creating a characteristic cuff at the ankles or wrists.
Lymphedema often causes asymmetrical swelling, and the hands or feet are commonly involved. The swelling may feel firm and may worsen throughout the day as fluid accumulates.
Pain and tenderness are common symptoms of lipedema, and many patients report that the affected areas are sensitive to pressure. In contrast, lymphedema is typically less painful, although patients may experience heaviness, tightness, or discomfort due to swelling.
Both conditions can cause enlargement of the legs or arms, which can make them appear similar. However, lipedema involves abnormal adipose tissue, while lymphedema involves fluid accumulation due to lymphatic dysfunction. Because awareness of lipedema has historically been limited, many patients are initially misdiagnosed with obesity or lymphedema.
Yes, treatment strategies differ because the conditions have different causes. Lipedema management may include compression therapy, lymphatic drainage, lifestyle measures, and in selected patients, lipedema reduction surgery using lymphatic-sparing liposuction techniques.
Lymphedema treatment typically focuses on improving lymphatic drainage, using therapies such as compression garments, manual lymphatic drainage, pneumatic compression therapy, and specialized physical therapy. In certain cases, surgical procedures may be considered.
Yes. In some patients, long-standing lipedema can eventually impair lymphatic drainage, leading to secondary lymphedema, a condition sometimes called lipo-lymphedema. In these cases, patients may experience features of both disorders, including abnormal fat deposits and fluid-related swelling.